delta dental application form
Male Married Widowed Civil Union Domestic Partnership Single Divorced Female Mailing. An application must be received by the 15 th of the month prior to your policy effective date.
Member Resources Delta Dental
Until you receive your username and.
. Have a question about coverage or looking for dental insurance. Dental Initial Credentialing Application Dental Initial Credentialing Application Ready to submit. An incomplete application could result in either a decline of application or delay in effective date.
Delta Dental PPO participation packet request. 800 403-6101 Online Enrollment Application Change Form Delta Dental of Washington offers the ability to view andor submit enrollment and most census changes in real time through the Delta Dental of Washington secured website. OR provide the full name of an already existing credentialed provider that we can.
We have made available for download important forms to ensure you have everything you need just a click away. Delta Dental HIPAA Form 14b ASO Groups. Required fields are starred and must be completed to ensure enrollment.
Group Information Change Request Form. Find the forms and resources to assist you in administering Delta Dental of Oklahoma benefit products and services. Please print clearly or type.
Get Cost by Provider or Procedure. Delta Dental reserves the right to change premium rates upon renewal of the policy. Delta Dental of Minnesota - Agent Quoting tools forms and resources.
Fill in each fillable area. Authorization To Release Protected Health Information. Complete section F before submitting to Delta Dental of Arizona.
Healthy Smile Healthy You enrollment form. PO Box 40384 Portland Oregon 97240-0384 Dental plans in Oregon provided by Oregon Dental Service dba Delta Dental Plan of Oregon. Find My Delta Dental.
Fees- the applicant will need to supply a Confidential Filed Fee CFF schedule with this application. Select your employers headerquarters or the. Delta Dental of Illinois EnrollmentChange of Status Form for Dental and Vision Policy APPLICANT Please type or print in black ink and complete the application in its entirety.
Complete the application Add a PracticeLocation to your Delta Dental Membership If youre already a Delta Dental Member Dentist and are adding an additional location to your membership follow these steps. Checklist for Delta Dental Credentialing. Application and Change Form for Individual Family Dental Insurance PO.
Box 981400 Boston Massachusetts 02298-1400 Please print or type. Locum Tenens Provider Form. Delta Dental is a Government contractor subject to the Section 4212 of the Vietnam Era Veterans Readjustment Assistance Act of 1974 as amended by the Jobs for Veterans Act of 2002 which requires Government contractors to take affirmative action to employ and advance in employment.
This means that the information you see on our website reflects current eligibility in our system. The national network of Delta Dental companies protects more smiles than any other insurance company. PDF forms may be downloaded.
Delta Dental PPO and Delta Dental Premier network dentists submit claim forms automatically on behalf of Delta Dental patients. Applications postmarked by the 10th of the month will become effective the 1st of the following month. 1 Disabled veterans A veteran who served on active duty in the US.
Print Your ID Cards. Removable Prosthodontics Assessment Form. Chat with a Customer Experience Specialist.
There are 3 available alternatives. Sign and date this form before submitting to Delta Dental of Arizona. You can download this form insert the necessary information.
Dentist Directory Update Form. Additional Information Form Facility Profile-Form helps with the CMS and DDPA requirements regarding information that is listed on the website. Typing drawing or capturing one.
Subscriber must be age 18 or older. Automatic Draft Authorization Form Employee Enrollment Form English Employee Enrollment Form Spanish General Change Form for Groups editable Application for Online Resources editable Business Forms for. Delta Dental Premier Network Forms - Professional Application Credentialing form Delta Dental Premier Dentists Agreement Ownership Control Form and W-9.
Here are a few quick. Delta Dental agrees to keep your coverage in force as long as you continue to pay the premiums on time and as long as you retain residency in the state of Massachusetts. Appeal Form - Information on how to appeal your claim.
Delta Dental HIPAA Form 14a Risk Groups. It takes approximately two weeks to process a complete Direct Electronic Access Agreement. ASO contract addendum for HIPAA privacy and security.
Sale of Practice Notification Form. Of the month and will be based upon Delta Dentals date of receipt and acceptance of this application. Connect with your Delta Dental to learn more.
Continuous Orthodontic Coverage Form for DeltaCare USA. To expedite your application please complete the fillable form and include your electronic signature or your Adobe digital ID signature. Review the Member Dentist Rules and Regulations Complete the application Non-Participating Provider Application.
Student Certification Form Use this form to certify dependents as college students Group Data Form. Make sure the data you fill in Delta Dental Credential Application Form For California is up-to-date and correct. Submit the signed form to your employer who will complete section F.
Click on the Sign tool and create a digital signature. Include the date to the sample using the Date function. Delta Dental of Illinois complies with applicable Federal civil rights laws and does not discriminate on the basis of sex sexual orientation race color religious creed national origin citizenship age physical or mental disability protected veteran status gender gender identity or expression marital status genetic information or any other characteristic protected by law.
DeltaCare USA participation packet request. Employer Subgroup Information Page and Application Addendum Individual Authorization Form. Were here to help.
With Delta Dental we keep you smiling. Dental plans in Alaska provided by Delta Dental of Alaska 60403711 120. Complete this form in full to ensure timely processing.
Enrollment ApplicationChange of Status Form Created Date. Mail this form to Delta Dental Mail. Certificate Of Coverage For Small Businesses.
Theres no hassle in working through claims saving you time and frustration. You also have the option to complete this application form using black or blue ink and include your handwritten signature. Automatic bank draft authorization for risk groups.
SIGN IN or REGISTER to access more tools. Healthy Smile Healthy You enrollment form Spanish. To access a dental claim form.
SECTION F - Employer Use Only. The NPI is part of the required credentialing material necessary for participating Delta Dental of Virginia dentists. Forms At Delta Dental we want to make selling our products as simple as possible.

Delta Dental Insurance Login Delta Dental
![]()
Affiliate Plans Delta Dental

Delta Dental Privacy Statement
![]()
Affiliate Plans Delta Dental
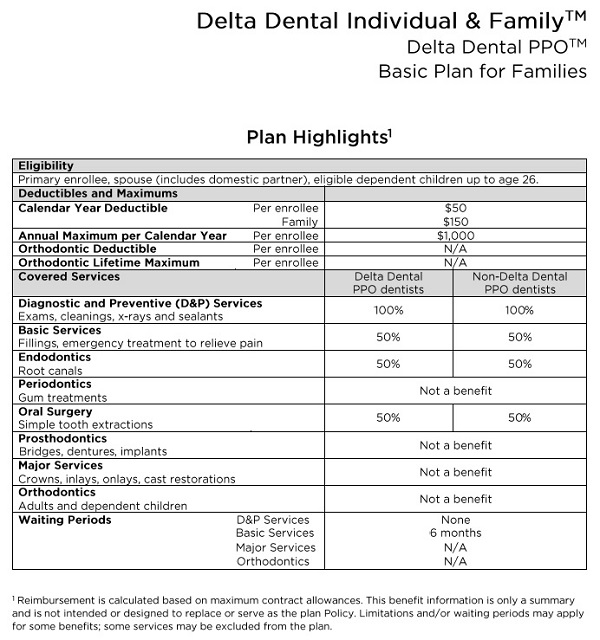
Delta Dental Individual Family Plans For 2019
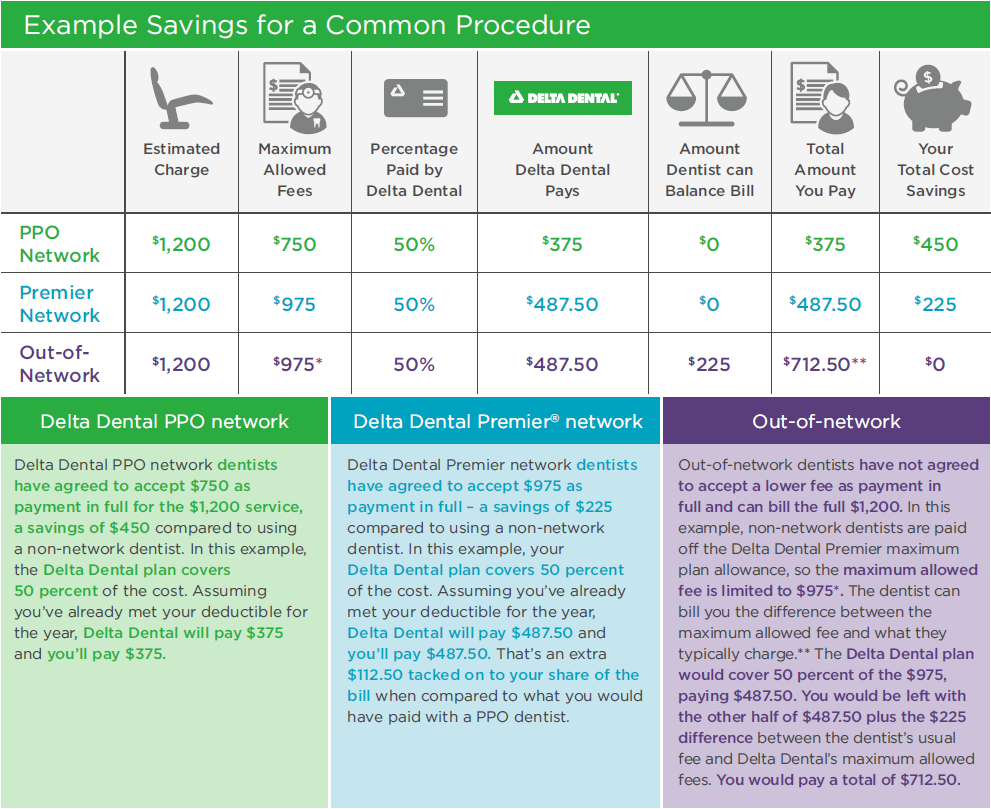
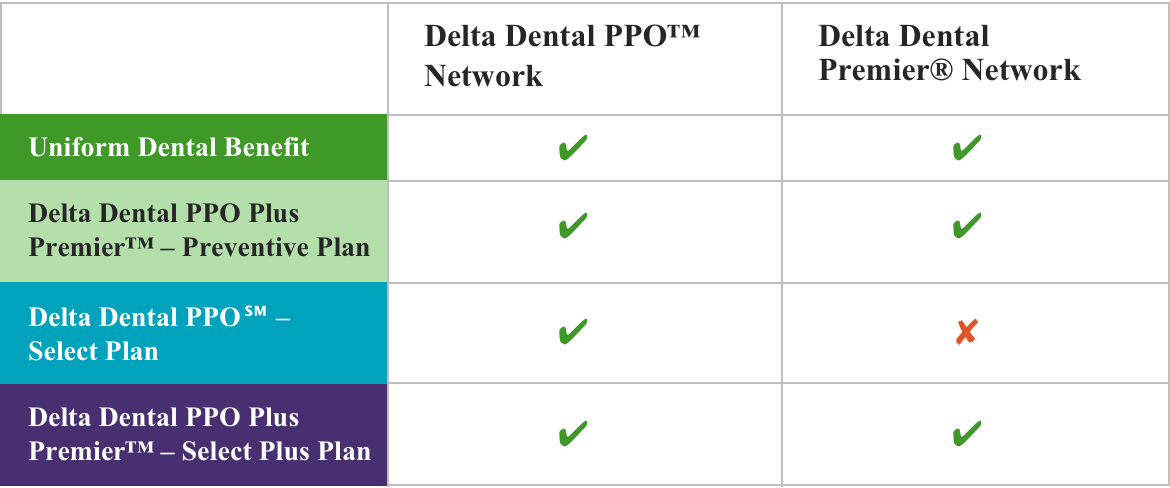
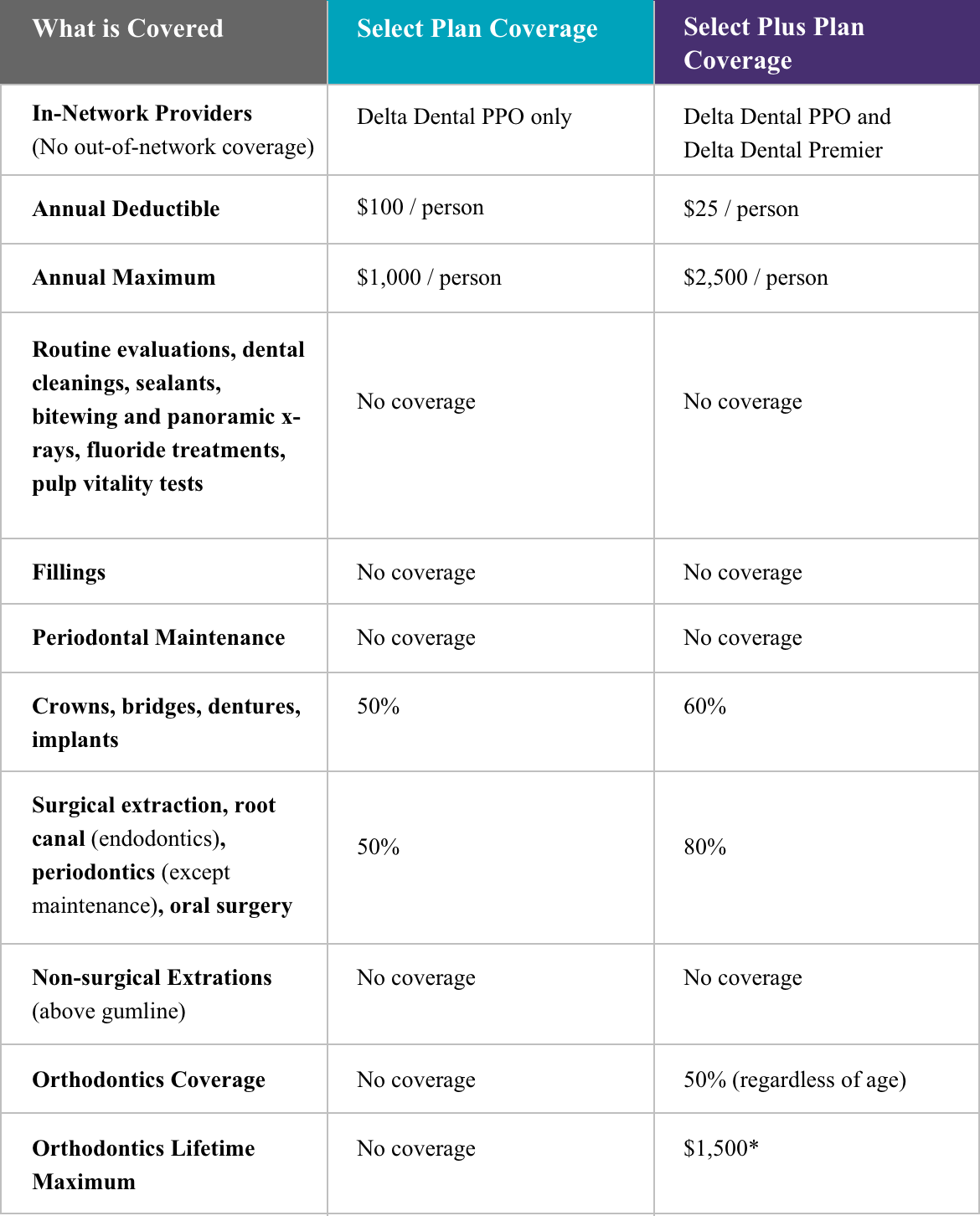
Ppo Vs Premier Dental Coverage Delta Dental Of Illinois

Employer Forms Resources Delta Dental Of Michigan
Dental City Of Lexington

In Network Dentist Benefits Out Of Network Dentist

Men By The Numbers Educational Infographic Dental Problems Informative
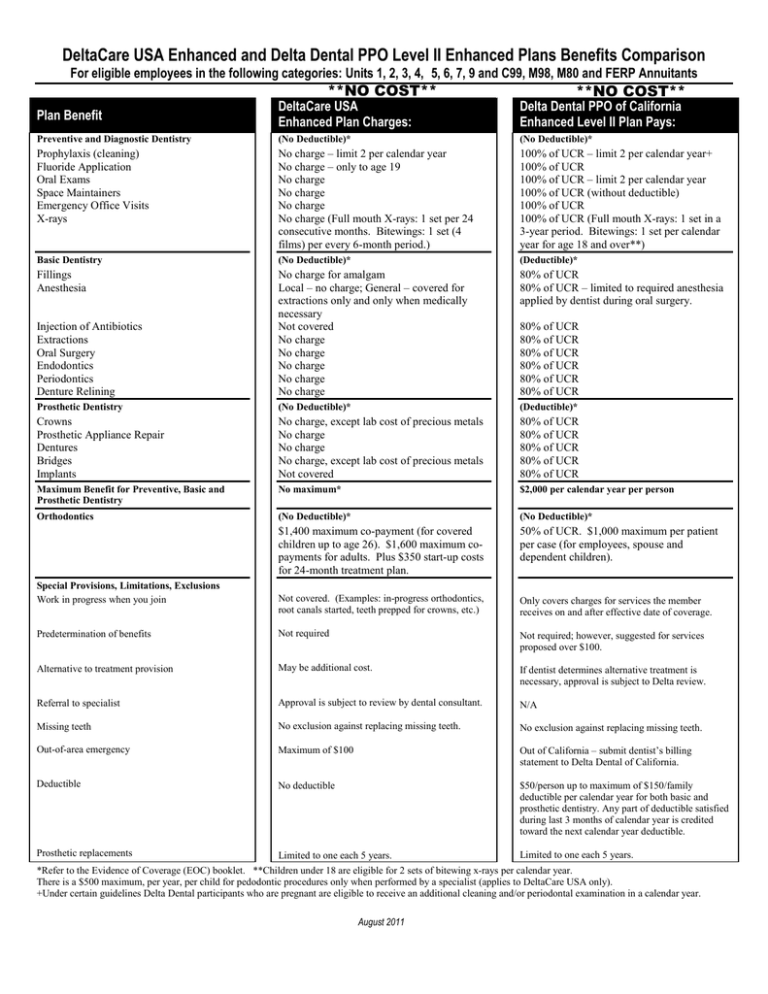
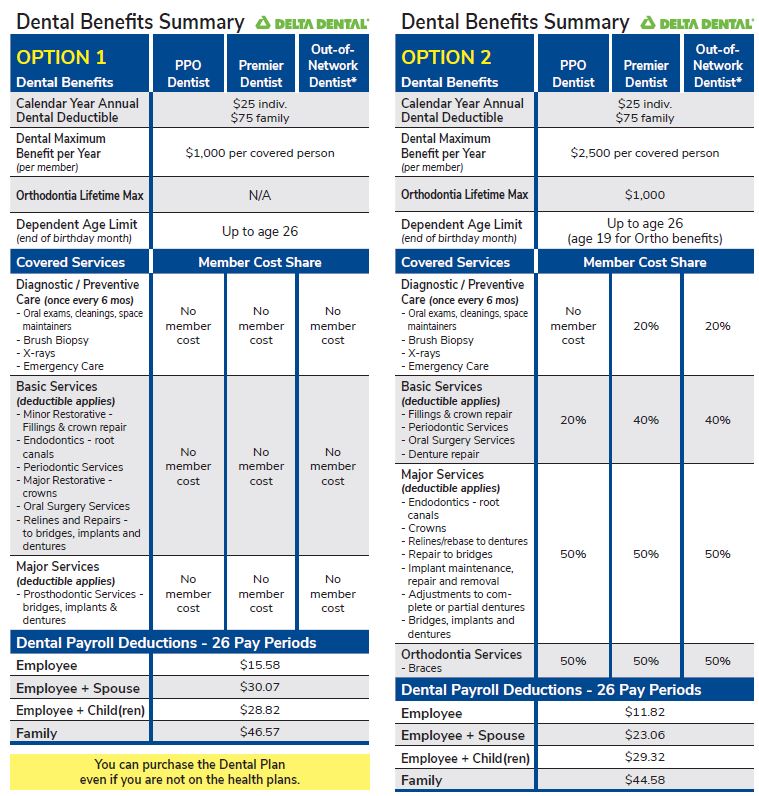
Deltacare Usa Enhanced And Delta Dental Ppo Level Ii Enhanced

Delta Dental Of Missouri Members Your Id Card Dental Missouri Delta

Why Choose Delta Dental Advantage Of Delta Dental
State Of Wisconsin Etf Delta Dental Of Wisconsin

Plan Documents
State Of Wisconsin Etf Delta Dental Of Wisconsin
![]()
Delta Dental Washington Healthplanfinder

About

Online Dental Insurance Tools Delta Dental Of Washington